
Recording of patient-reported outcome measures for anxiety disorders and depression in English primary care
Abstract
TODO
Keywords: patient-reported outcome measures, anxiety disorders, depression, primary care, SNOMED CT, electronic health records
Introduction
Anxiety disorders and depression are leading contributors to disease burden in England. The nationally representative Adult Psychiatric Morbidity Survey (APMS) found that the prevalence of common mental health conditions in adults increased from 18.9% in 2014 to 22.6% in 2023/24 (Morris et al. 2025). In the most recent 2023/24 survey, generalised anxiety disorder (7.5%) and depression (3.8%) were the most prevalent conditions in adults (Morris et al. 2025). Primary care is the main point of contact for people with anxiety disorders and depression in England, with 13.2% of adults with common mental health conditions having spoken to their GP about mental health in the past year (Morris et al. 2025). Many also receive support through NHS Talking Therapies for Anxiety and Depression (National Collaborating Centre for Mental Health 2024). In both settings, structured assessment of symptom severity is central to identifying appropriate treatment, monitoring progress, and guiding clinical decisions (National Institute for Health and Care Excellence 2020, 2022).
Patient-reported outcome measures (PROMs) are self-completed questionnaires that quantify symptom severity and are widely used for this purpose in English primary care, where their adoption has been shaped by clinical guidelines and financial incentives. The National Institute for Health and Care Excellence (NICE) recommends validated measures to assess severity and guide treatment decisions (National Institute for Health and Care Excellence 2020, 2022), and the Quality and Outcomes Framework (QOF) created financial incentives for GPs between 2006 and 2013 to record structured severity assessments at diagnosis and follow-up (Kendrick et al. 2015). For depression, the British Medical Association recommended three tools for primary care use (2006): the Patient Health Questionnaire-9 (PHQ-9, Kroenke et al. 2001), the Beck Depression Inventory (BDI-II, Beck et al. 1996), and the Hospital Anxiety and Depression Scale (HADS-D, Zigmond and Snaith 1983). For anxiety disorders, the Generalised Anxiety Disorder 7-item scale (GAD-7, Spitzer et al. 2006) is widely used for severity assessment, with the GAD-2 recommended as an initial screening tool (Plummer et al. 2016; National Institute for Health and Care Excellence 2020). Disorder-specific measures are additionally recommended for panic disorder, obsessive compulsive disorder, and posttraumatic stress disorder (National Collaborating Centre for Mental Health 2024). As yet, it is unknown which PROMs are most commonly recorded nationally and how this has changed over time.
Given the availability of national SNOMED CT code usage data through the opencodecounts R package (Tamborska et al. 2025), PROMs recording patterns can be examined at population scale across all English general practices, without requiring access to individual patient-level data. Importantly, patterns of SNOMED CT code usage reflect both clinical activity and the policy incentives that shape it, meaning that national code usage data can capture how PROM recording has changed alongside revisions to QOF requirements (Tamborska et al. 2025). Describing which PROM codes are in use, how frequently they appear, and how usage has changed over time is an important step towards building research codelists that accurately capture intended clinical activity and planning feasible patient-level studies (Matthewman et al. 2024).
The present study described national patterns and trends in the recording of PROMs for anxiety disorders and depression in English primary care, using national SNOMED CT code usage data from 2011 to 2025. The first aim was to characterise which PROM codes are recorded in routine primary care and their relative frequency across the study period. The second aim was to examine how PROM recording has changed over time, including any changes associated with revisions to QOF requirements.
Methods
Data sources
Clinical code usage in primary care: We used publicly available SNOMED CT code usage data from NHS England accessed via the opencodecounts R package (Tamborska et al. 2025). OpenCodeCounts is an interactive tool and R package that provides access to annual summaries of clinical code usage in England, which includes SNOMED CT codes recorded in primary and ICD-10/OPCS-4 codes recorded in secondary care (Tamborska et al. 2025) The SNOMED CT usage data are published by NHS England1, and cover the period from August 2011 to July 2025. The usage count reflects how many times each listed SNOMED CT code was added to a GP patient record in England during the annual reporting period, with counts rounded to the nearest 10. Each yearly data point is labelled by its end date (e.g., “July 2024” covers the period from 1 August 2023 to 31 July 2024). Prior to 2019, data were submitted in Read v2 or CTV3 format and have been mapped to SNOMED CT, which may affect the comparability of counts across the full study period. Since counts are aggregated, they reflect instances of code use rather than distinct patients, as a given code may be added to a patient record more than once within a single consultation or reporting period.
Codelist development
Two codelists covering PROMs for anxiety disorders and depression were developed iteratively, following published guidance on codelist development and sharing (Matthewman et al. 2024). We reviewed NICE guidelines (National Institute for Health and Care Excellence 2020, 2022) and the NHS Talking Therapies manual (National Collaborating Centre for Mental Health 2024) for search terms. We also reviewed existing NHS Primary Care Domain Reference Set2 (NHS Digital 2025b, 2025a) and consulted a GP to identify additional clinically relevant search terms not captured through these sources.
Codelists were created and published on OpenCodelists3, an open-access platform for creating and sharing clinical codelists. Searches were conducted in R using all SNOMED CT descriptions from the opencodecounts R package (Tamborska et al. 2025), with case-insensitive matching and different spelling variants. Terms included PROM names (e.g., PHQ-9, GAD-7), condition terms, and broader assessment and screening terms (see Supplementary Table 1 for the full list of search terms). The codelists, including methodology and all search terms, are provided with the two final codelists we used in this study (Ojedele 2025b, 2025a).
Data analyses
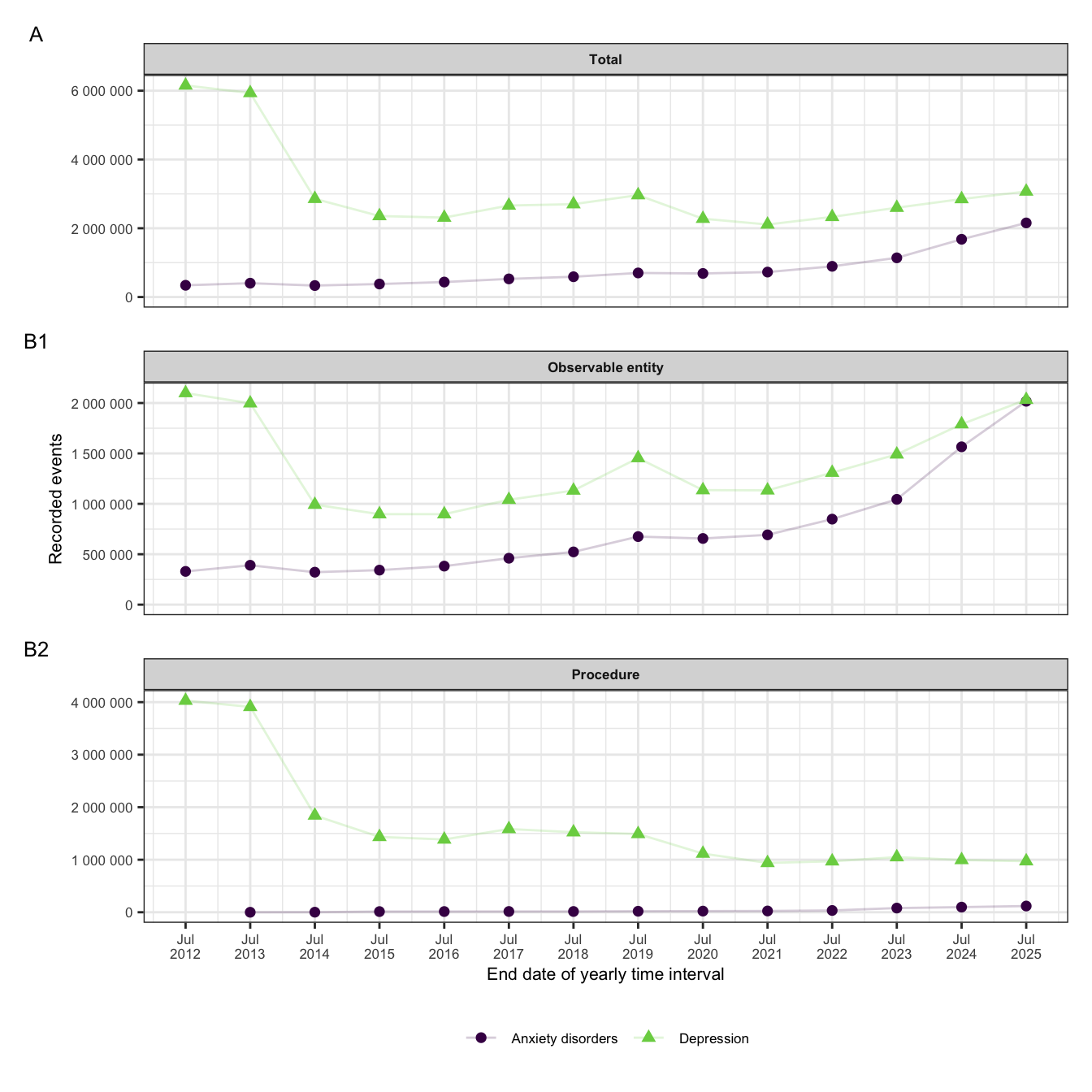
Using the final depression and anxiety disorder PROM codelists, we conducted descriptive analyses of national SNOMED CT usage patterns over time. Annual usage counts were extracted for all codes included in each codelist and summarised by reporting year and condition group Counts were also broken down by semantic tag (“Observable entity”, “Procedure”, and all other tags) to distinguish recorded PROM scores from recorded assessment activity. Yearly trajectories of total usage counts were plotted to examine trends over time and identify changes in coding patterns. Codes were ranked by their aggregate usage count within each codelist to identify the five most frequently recorded depression-related and anxiety disorder-related PROM codes. For each of these codes, we calculated the proportion of total codelist usage represented by that code. All analyses were descriptive and conducted using R with the opencodecounts package (Version 0.5.0, Tamborska et al. 2025), and analysis code is openly available at https://github.com/bennettoxford/mental-health-open-data.
Results
Yearly recorded events for PROMs codes for anxiety disorders and depression are shown in Figure 1.
The five most frequently recorded SNOMED CT PROMs codes for each codelist are summarised in Table 1.
| SNOMED code | Description | Semantic tag | Usage | |
|---|---|---|---|---|
| Anxiety disorders | ||||
| 445455005 | GAD-7 score | Observable entity | 7,548,940 | 68.7% |
| 836571000000106 | GAD-2 score | Observable entity | 1,837,830 | 16.7% |
| 401319005 | HADS anxiety score | Observable entity | 764,990 | 7.0% |
| 908501000000101 | Anxiety screening | Procedure | 360,565 | 3.3% |
| 836551000000102 | GAD-2 assessment | Assessment scale | 123,970 | 1.1% |
| Depression | ||||
| 200971000000100 | Depression screening using questions | Procedure | 22,339,530 | 51.7% |
| 720433000 | PHQ-9 score | Observable entity | 18,131,670 | 42.0% |
| 401320004 | HADS depression score | Observable entity | 829,530 | 1.9% |
| 171207006 | Depression screening | Procedure | 724,300 | 1.7% |
| 450320001 | EPDS score | Observable entity | 172,690 | 0.4% |
| Note. GAD = Generalized Anxiety Disorder; HADS = Hospital Anxiety and Depression Scale; PHQ = Patient Health Questionnaire; EPDS = Edinburgh Postnatal Depression Scale. Percentage usage of PROMs calculated separately for anxiety disorders and depression. | ||||
Discussion
TODO
Conclusion
TODO
Funding
This project is funded by the Wellcome Trust (317455/Z/24/Z). The views expressed are those of the authors and not necessarily those of the Wellcome Trust or NHS England.
References
Beck, Aaron T., R. A. Steer, and G. K. Brown. 1996. Beck Depression Inventory–II Manual. 2nd ed. Hartcourt Brace.
British Medical Association. 2006. Revisions to the GMS Contract, 2006/07. Delivering Investment in General Practice.
Kendrick, Tony, Beth Stuart, Colin Newell, Adam W. A. Geraghty, and Michael Moore. 2015. “Did NICE Guidelines and the Quality Outcomes Framework Change GP Antidepressant Prescribing in England? Observational Study with Time Trend Analyses 2003–2013.” Journal of Affective Disorders 186 (November): 171–77. https://doi.org/10.1016/j.jad.2015.06.052.
Kroenke, Kurt, Robert L Spitzer, and Janet B W Williams. 2001. “The PHQ-9: Validity of a Brief Depression Severity Measure.” Journal of General Internal Medicine 16 (9): 606–13. https://doi.org/10.1046/j.1525-1497.2001.016009606.x.
Matthewman, Julian, Kirsty Andresen, Anne Suffel, et al. 2024. “Checklist and Guidance on Creating Codelists for Electronic Health Records Research.” NIHR Open Research 4 (April): 20. https://doi.org/10.3310/nihropenres.13550.1.
Morris, Sarah, Suzanne Hill, Traolach Brugha, and Sally McManus, eds. 2025. Adult Psychiatric Morbidity Survey- Survey of Mental Health and Wellbeing, England, 2023/4. https://doi.org/10.13140/RG.2.2.24367.39840.
National Collaborating Centre for Mental Health. 2024. NHS Talking Therapies for Anxiety and Depression Manual. https://www.england.nhs.uk/publication/the-improving-access-to-psychological-therapies-manual/.
National Institute for Health and Care Excellence. 2020. Generalised Anxiety Disorder and Panic Disorder in Adults: Management. NICE Clinical Guideline CG113. NICE. https://www.nice.org.uk/guidance/cg113.
National Institute for Health and Care Excellence. 2022. Depression in Adults: Treatment and Management. NICE Clinical Guideline NG222. NICE. https://www.nice.org.uk/guidance/ng222.
NHS Digital. 2025a. Primary Care Domain Reference Set: Anxiety Screening Codes. V. 20250912. Released. https://www.opencodelists.org/codelist/nhsd-primary-care-domain-refsets/anxscrn_cod/20250912/.
NHS Digital. 2025b. Primary Care Domain Reference Set: Depression Screening Codes. V. 20250912. Released. https://www.opencodelists.org/codelist/nhsd-primary-care-domain-refsets/depscrn_cod/20250912/.
Ojedele, Lola. 2025a. OpenCodelists: Patient-Reported Outcome Measures for Anxiety Disorders. V. 387cdfd9. Released. https://www.opencodelists.org/codelist/user/Lola_O/patient-reported-outcome-measures-for-anxiety-disorders/387cdfd9/.
Ojedele, Lola. 2025b. OpenCodelists: Patient-Reported Outcome Measures for Depression. V. 2ceb2c72. Released. https://www.opencodelists.org/codelist/user/Lola_O/patient-reported-outcome-measures-for-depression/2ceb2c72/.
Plummer, Faye, Laura Manea, Dominic Trepel, and Dean McMillan. 2016. “Screening for Anxiety Disorders with the GAD-7 and GAD-2: A Systematic Review and Diagnostic Metaanalysis.” General Hospital Psychiatry 39 (March): 24–31. https://doi.org/10.1016/j.genhosppsych.2015.11.005.
Spitzer, Robert L, Kurt Kroenke, Janet B. W. Williams, and Bernd Löwe. 2006. “A Brief Measure for Assessing Generalized Anxiety Disorder: The GAD-7.” Archives of Internal Medicine 166 (10): 1092. https://doi.org/10.1001/archinte.166.10.1092.
Tamborska, Arina Anna, Rose Higgins, Yamina Boukari, et al. 2025. “OpenCodeCounts: An Open-Access, Interactive Online Tool and R Package for Analysing Clinical Code Usage in England.” Pre-published October 15. https://doi.org/10.1101/2025.10.14.25338005.
Zigmond, A. S., and R. P. Snaith. 1983. “The Hospital Anxiety and Depression Scale.” Acta Psychiatrica Scandinavica 67 (6): 361–70. https://doi.org/10.1111/j.1600-0447.1983.tb09716.x.
Footnotes
https://digital.nhs.uk/data-and-information/publications/statistical/mi-snomed-code-usage-in-primary-care↩︎
https://digital.nhs.uk/data-and-information/data-collections-and-data-sets/data-collections/quality-and-outcomes-framework-qof/quality-and-outcome-framework-qof-business-rules/primary-care-domain-reference-set-portal↩︎